Samantha K. Micsinszki, Alexis Buettgen, Gillian Mulvale, Sandra Moll, Michelle Wyndham-West, Emma Bruce, Karlie Rogerson, Louise Murray-Leung, Robert Fleisig, Sean Park and Michelle Phoenix
This blog post is based on the Evidence & Policy article, ‘Creative processes in co-designing a co-design hub: towards system change in health and social services in collaboration with structurally vulnerable populations’, part of the Special Issue on Creativity and Co-production.
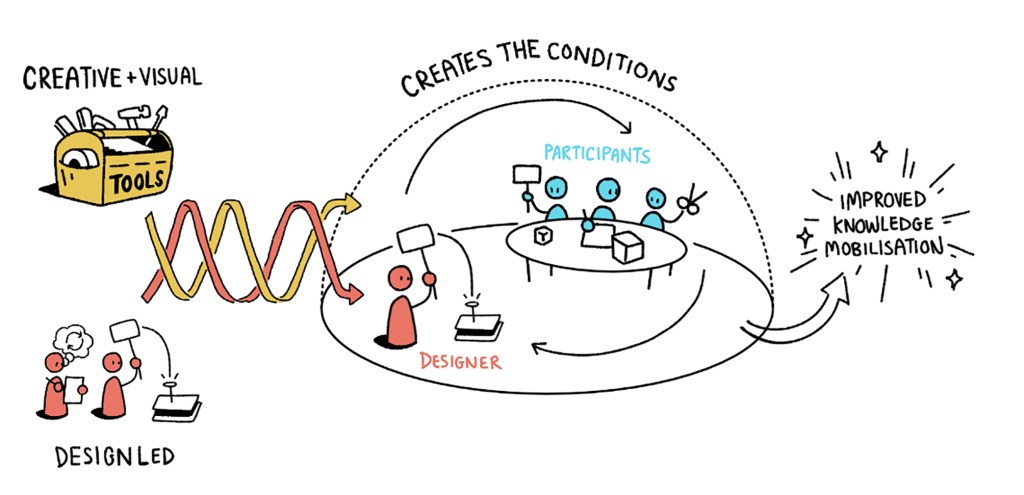
What creative tools can we use to disrupt the status quo and create truly inclusive health and social services? Co-designing evidence and policy change in collaboration with health and social service users and their families is part of an exciting and growing international movement. In our Evidence & Policy article, ‘Creative processes in co-designing a co-design hub: towards system change in health and social services in collaboration with structurally vulnerable populations’, we highlight how our interdisciplinary team of researchers, trainees and lived experience experts engaged in a three-year collaborative process to promote engagement, education, and innovation in equity-based co-design. This article is part of a special issue on creativity and co-production that highlights how collaborative practices, such as co-design and co-production, can be elevated using creative devices and tools (e.g., imagination, storytelling, art etc.) to create a shared language, build relationships, and make meaning.
Co-design approaches take a person-centered perspective, utilizing a design lens to develop solutions to problems in collaboration with lived experience experts. This approach can redistribute power when we meaningfully and effectively engage individuals and communities who experience structural vulnerabilities that affect their health and well-being (e.g., racism, sexism, ableism, colonialism). In other words, how do we ensure that diverse experiences are included and that co-design processes lead to lasting system change?
Continue reading